
Dating Methods discussed below:
Last Menstrual Period (LMP)
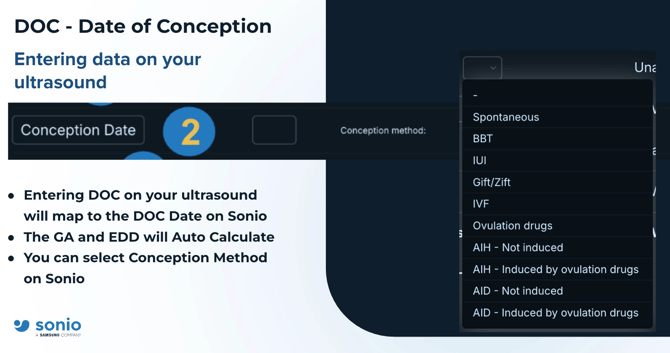
Date of Conception
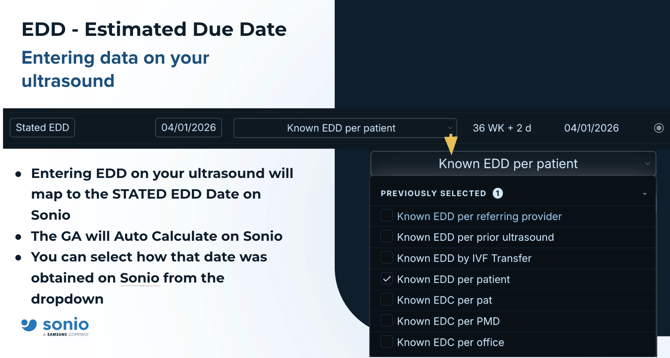
Stated EDD
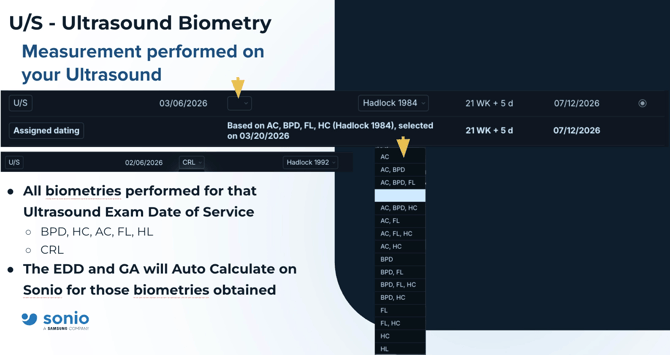
U/S (based on Biometries)
Hadlock 1984/1985/1991
Last Menstrual Period (LMP)
The first day of a patient’s last menstrual period (LMP) is the cornerstone of pregnancy dating because it provides a clear, documented starting point for calculating your estimated due date (EDD).
Why the LMP Date Matters
- Gestational Age: Doctors measure pregnancy in weeks starting from the first day of your LMP, not the date of conception. This means you are technically "two weeks pregnant" before the baby is even conceived.
- Scheduling Screenings: Accurate dating ensures that critical tests—like first-trimester screenings for genetic conditions—are performed at the correct developmental window.
- Monitoring Growth: It provides a baseline to see if the fetus is growing at the expected rate.
- Managing Risks: Knowing exactly how far along you are is vital for identifying preterm labor or determining if a pregnancy is post-term (overdue), which may require medical induction.
How the Calculation Works
The standard method, known as Naegele's Rule, estimates your due date by:
- Identifying the first day of your LMP.
- Subtracting 3 months.
- Adding 7 days and 1 year.
Is It Always Accurate?
While LMP is the standard, it assumes a regular 28-day cycle with ovulation on day 14. If your cycles are irregular or you conceived while on birth control, your doctor will likely use an early ultrasound (usually between 8–12 weeks) to confirm or adjust the date. First-trimester ultrasounds are currently considered the most accurate way to establish a due date.
ACOG Dating Clinical Guidelines - LMP
Conception Date
In medical settings, ultrasound uses fetal measurements to determine gestational age (weeks since your last period), but this is directly tied to the conception date (the day the egg was fertilized).
Why Conception Date Matters in Ultrasound
- Defining the "True" Age: While doctors count from your LMP, the baby’s actual age (conceptional age) starts at fertilization, usually about two weeks later. Ultrasound is the most reliable way to estimate this when you don't know your exact ovulation day.
- Adjusting the Due Date: If your ultrasound shows a significant "lag" or "lead" compared to your LMP (usually more than 5–7 days in the first trimester), doctors use the ultrasound’s estimated conception date to reset your official due date.
- Assessing Health Risks: A discrepancy where ultrasound age is much "behind" the expected LMP age can sometimes indicate a higher risk of pregnancy loss.
- Assisted Reproduction (IVF): For IVF pregnancies, the exact conception date is known. Ultrasound is used to verify that the embryo is growing at the precise rate expected for its age, providing the "gold standard" for dating accuracy.
Accuracy of Ultrasound Estimates
Ultrasound is most accurate at pinpointing the conception window during the first trimester (6–12 weeks).
- First Trimester: Accuracy within ±5–7 days.
- Second Trimester: Accuracy drops to ±10–14 days.
- Third Trimester: Accuracy can be off by ±21–30 days, as individual genetics begin to influence baby size more than age does.
How to Find Your Conception Date from an Ultrasound
If you have an ultrasound report, you can roughly find your conception date by:
- Identifying the gestational age provided (e.g., 10 weeks).
- Subtracting 2 weeks to find the fetal/conceptional age (e.g., 8 weeks).
- Counting back that many weeks from the date of the scan.
Stated EDD (Estimated Due Date)
The Estimated Due Date (EDD) calculated by ultrasound is considered the most accurate method for dating a pregnancy, often superseding dates based on your last period (LMP). Establishing an accurate EDD early is vital for managing clinical care and ensuring a healthy delivery.
Why Ultrasound EDD is Critical
- Refining Timing: Since many people have irregular cycles or do not remember their LMP, ultrasound provides a definitive "best obstetric estimate".
- Screening Accuracy: Critical tests, such as nuchal translucency screenings for chromosomal conditions, must be performed during very specific weeks to be valid.
- Growth Monitoring: An accurate due date allows doctors to correctly identify if a baby is too small (Growth Restriction) or too large (Macrosomia), which can be missed if the dating is off.
- Avoiding Risks: Precise dating helps prevent unnecessary medical inductions for being "overdue" and ensures that babies born early receive the correct level of preterm care.
Accuracy by Trimester
The earlier an ultrasound is performed, the more reliable the EDD it provides:
- First Trimester (6–13 weeks): The most accurate, with a margin of error of only ±5–7 days.
- Second Trimester (14–22 weeks): Margin of error increases to ±7–14 days.
- Third Trimester (28 weeks+): Least accurate, with a margin of error up to ±21–30 days. At this stage, scans are used to check growth and fluid, not to change the due date.
Clinical Rules for Changing Your Due Date
Doctors typically only change your "official" due date if the ultrasound measurement differs from your LMP by a certain number of days:
Before 9 weeks | Difference > 5 days
9–14 weeks | Difference > 7 days
16–22 weeks | Difference > 10 days
22–28 weeks | Difference > 14 days
A pregnancy without an ultrasound confirmation before 22 weeks is considered sub-optimally dated by the American College of Obstetricians and Gynecologists (ACOG).
In obstetric care, a CRL ultrasound EDD—specifically from the first trimester—is the "gold standard" for dating a pregnancy. Once established, it is rarely changed because early measurements are the most accurate reflection of a baby's age.
Why the First Ultrasound EDD Stays Fixed
- Biological Consistency: In the first trimester (up to 13 6/7 weeks), all embryos grow at nearly the same rate. This makes the Crown-Rump Length (CRL) measurement highly reliable, with an error margin of only ±3–7 days.
- Reference for Growth: Later in pregnancy, babies begin to grow at different speeds due to genetics and environment. If a 30-week ultrasound gives a different EDD, doctors do not change the original date; instead, they use the discrepancy to check if the baby is growing too slowly (growth restriction) or too quickly.
- Clinical Anchor: The first accurate EDD is used to schedule all future care, including the anatomy scan (18–22 weeks) and decisions about medical induction if you go past your due date.
When the "Prior" EDD Might Be Ignored
While the earliest scan is prioritized, doctors may re-evaluate the EDD in specific scenarios:
- "Suboptimal" Dating: If the first ultrasound was done late (after 22 weeks), it is considered suboptimally dated because the error margin increases to ±2–3 weeks.
- Significant Discrepancy: If a current scan shows a massive difference (e.g., more than 21 days in the third trimester) from the established date, doctors may investigate for growth disorders rather than just changing the date.
- Assisted Reproduction (IVF): If you had IVF, the embryo transfer date provides the absolute EDD, which overrides any ultrasound measurement.
U/S (Current EDD based of Biometries)
Determining the Estimated Due Date (EDD) through fetal biometry—measuring specific parts of the baby’s body—is the most reliable way to assess gestational age when a first-trimester "crown-rump length" scan is unavailable.
Key Biometric Measurements
To calculate the EDD after the first trimester, sonographers measure four primary markers:
- Biparietal Diameter (BPD): The width of the baby’s head from ear to ear.
- Head Circumference (HC): The total distance around the head; highly accurate for dating in the second trimester.
- Abdominal Circumference (AC): Used primarily to estimate fetal weight and health, rather than just age.
- Femur Length (FL): The length of the thigh bone, which is a reliable indicator of longitudinal growth.
Why Biometry-Based EDD is Important
- Identifying Growth Issues: By comparing biometric measurements to a known EDD, doctors can diagnose Intrauterine Growth Restriction (IUGR) if the baby measures much smaller than expected.
- Standardizing Care: It creates a "biological age" that allows clinicians to time interventions, such as steroid injections for lung development if preterm birth is suspected.
- Compensating for Missing Data: For patients with irregular periods or those who seek late prenatal care, biometry provides the only scientific basis for a due date. [12]
Accuracy of Biometry
As pregnancy progresses, the "margin of error" for biometry-based EDD increases because babies grow at different rates due to genetics:
- 14–22 weeks: Accurate within ±7–10 days.
- 22–28 weeks: Accurate within ±10–14 days.
- After 28 weeks: Accurate only within ±21–30 days.
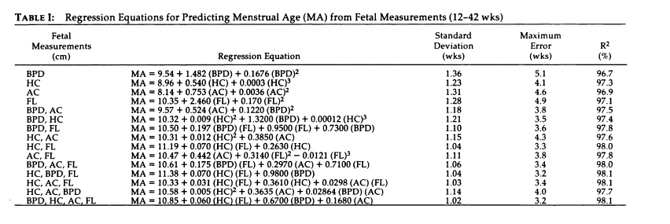
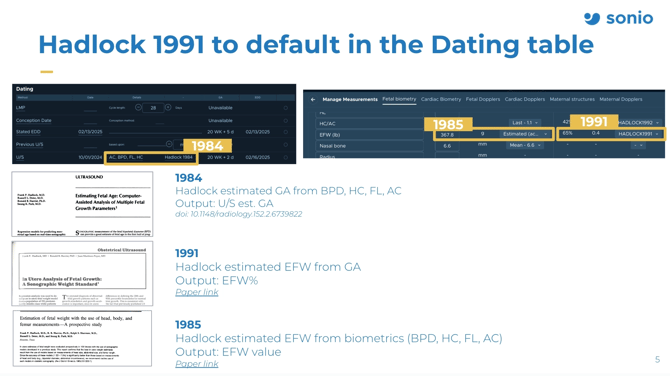
HADLOCK 1984 GA Calc, 1985 EFW CALC, 1991 EFW revised percentile Calc
Hadlock 1984
To estimate GA from US biometries (all or combination of BPD, HC, FC, FL) - doi: 10.1148/radiology.152.2.6739822
Hadlock 1985
To estimate EFW from 3 parameter (HC, AC, FL) or 4 parameters (BPD, HC, AC, FL) - Hadlock 1985 publication
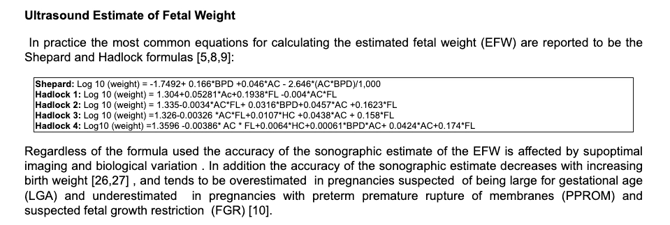
Hadlock 1991
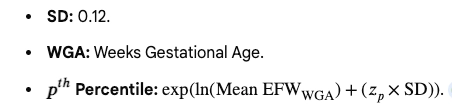
To estimate EFW from GA - Output is EFW percentile - Hadlock 1991 publication
Optimal Equation: The 1991 paper identified a regression equation Log n weight (g) = 0.578 + 0.332 MA- 0.00354 MA2 , where MA is menstrual age (standard deviation= 0.12, R2 = 99.1%). to determine percentiles directly, which is preferred over lookup tables to reduce FGR under diagnosis.

If there's an EFW discrepancy between Sonio and your ultrasound machine, click here for guidance